
Posts Shortcodes
You can show the posts with Porto Blog, Porto Recent Posts shortcodes.
Recent
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar! Insulin – The Body’s Nutrient Gateway! Most people think insulin exists only to lower blood... read more

Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal? Walk through any supermarket or browse social media,... read more

Milk And Paneer Vs Soya, Soya Milk And Tofu Proteins!
Milk Protein Vs Soya Protein: Which Is The Better Protein? Protein is one of the most important nutrients for maintaining... read more

Protein: The Forgotten Nutrient in Indian Diets!
Are Proteins The Most Neglected Nutrient In our Diets? Protein is one of the three major nutrients our body needs... read more

Healthy Nutrition for Pre-Teens!
Building Foundations for Lifelong Health! The pre-teen years (roughly 9–12 years of age) are a period of rapid physical and... read more

Can Exercise Turn Back the Clock on Your Heart?
What Consistent Exercise Can To Your Heart Health! We often think of aging as an unstoppable process. As the years... read more

The New Weight Loss Drugs — Science, Benefits And Misuse!
Benefits As Medical Treatment And Dangers Of Unethical, Casual Use! A new class of medicines originally developed for diabetes has... read more
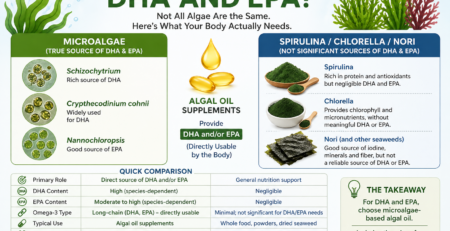
Which Algae Provide DHA And EPA?
Microalgae, Spirulina, Chlorella And Nori! Why Most ‘Algae Superfoods” Don’t Meet Your Omega-3 Needs? Most algae are promoted as nutritional... read more
Timeline
August 2026
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar!
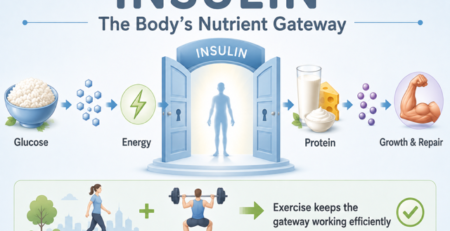
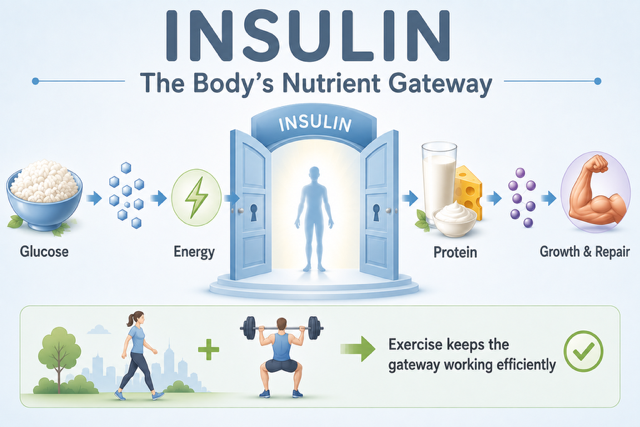
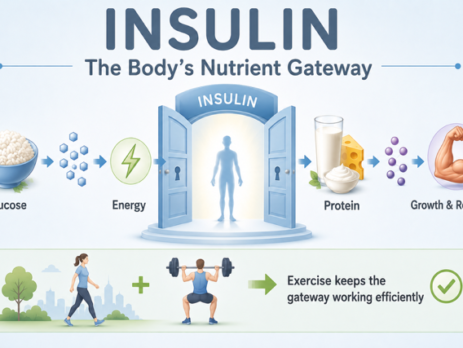
Insulin – The Body’s Nutrient Gateway!
Most people think insulin exists only to lower blood sugar.
In reality, insulin has a much broader and far more important job.
Its main role is to help nutrients move from the bloodstream into body cells where they can be used or stored.
You can think of insulin as the body’s gateway hormone.
Without insulin, many cells cannot efficiently receive the nutrients they need.
Gateway For Glucose
After eating carbohydrates, digestion releases glucose into the bloodstream.
Blood glucose rises.
The pancreas responds by releasing insulin.
Insulin acts like a key that unlocks the doors of muscle cells and fat cells.
Glucose then enters these cells where it can be:
• used immediately to produce energy,
• stored as glycogen in muscles and the liver,
• or, when energy intake greatly exceeds requirements, eventually converted into body fat.
Without sufficient insulin—or when the body’s cells become resistant to insulin—glucose remains in the bloodstream and blood sugar rises.
Gateway For Amino Acids
The story is different after eating proteins.
Proteins are broken down into amino acids.
These amino acids also stimulate insulin release.
But this time insulin is not trying to lower blood sugar.
Instead, insulin helps amino acids enter muscle cells and other body tissues.
Once inside the cells, these amino acids are used to:
• build new muscle protein,
• repair damaged tissues,
• produce enzymes,
• manufacture hormones,
• support immune function.
Here, insulin functions as a growth and repair hormone rather than a glucose-lowering hormone.
Milk Demonstrates Both Roles Beautifully
Milk naturally contains both lactose and high-quality proteins.
The lactose produces a modest rise in blood glucose.
The proteins stimulate insulin through their amino acids.
Consequently, milk illustrates both major functions of insulin simultaneously.
Insulin helps glucose enter cells.
At the same time, it helps amino acids enter muscles for repair and maintenance.
Very few foods demonstrate both roles so clearly.
Exercise Makes The Gateway Work Better
Exercise opens another fascinating chapter.
When muscles contract during walking or strength training, they become much more responsive to insulin.
In other words, the gateway becomes easier to open.
The same amount of insulin can move more glucose and amino acids into muscle cells.
As a result:
• blood sugar rises less after meals,
• less insulin is needed,
• muscles receive more nutrients,
• muscle maintenance improves,
• metabolic health becomes better.
This is why regular physical activity improves insulin sensitivity.
When The Gateway Becomes Rusty
In insulin resistance, the gateway no longer responds efficiently.
The pancreas has to produce more and more insulin to achieve the same effect.
Over time, blood glucose begins to rise.
This is one of the earliest steps in the development of type 2 diabetes.
Fortunately, weight loss, regular walking, strength training and a healthy diet can often restore much of the gateway’s efficiency.
The Take-Home Message
Insulin is much more than a blood sugar hormone.
It is the body’s nutrient gateway.
It allows glucose to enter cells for energy.
It allows amino acids to enter cells for growth and repair.
Healthy muscles respond well to insulin.
Regular exercise keeps this gateway working efficiently.
Understanding insulin in this way makes it much easier to understand diabetes, muscle health, healthy ageing and nutrition.
Related article:
July 2026

Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron and nachani (ragi) as the ideal calcium-rich grain.
The truth is that no single grain is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends on your overall diet, health goals and the way the grain is processed and prepared.
Comparison of Common Indian Cereals
***
Which Is the Healthiest Indian Cereal: Wheat, Khapli Wheat, Jowar, Bajri or Nachani?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli (Emmer) wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron, and nachani (ragi) as the ideal calcium-rich cereal.
The reality is more balanced. No single cereal is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends not only on the grain itself but also on your overall diet, health goals and how the grain is processed and prepared.
Comparison of Common Indian Cereals:
Whole Wheat
Glycemic Index: 50–60
Key Nutritional Strengths: Protein, fibre, B vitamins, magnesium, zinc and selenium.
Major Antioxidants: Ferulic acid, phenolic acids and lignans.
Khapli Wheat
Glycemic Index: 40–50
Key Nutritional Strengths: More fibre, slightly more protein, iron, magnesium and zinc than modern wheat.
Major Antioxidants: Polyphenols, lutein, carotenoids and ferulic acid.
Jowar
Glycemic Index: 55–65
Key Nutritional Strengths: Protein, fibre, magnesium, phosphorus and potassium.
Major Antioxidants: Anthocyanins, flavonoids, phenolic acids and tannins.
Bajri
Glycemic Index: 50–55
Key Nutritional Strengths: Protein, fibre, iron, magnesium and phosphorus.
Major Antioxidants: Phenolic acids, flavonoids and phytosterols.
Nachani (Ragi)
Glycemic Index: 60–70†
Key Nutritional Strengths: Exceptionally rich in calcium, fibre, magnesium and potassium.
Major Antioxidants: Polyphenols, ferulic acid, catechins and tannins.
Approximate glycemic index values that vary with processing and cooking.
Finely ground nachani (ragi) flour may have a higher glycemic index than commonly believed.
What Makes Each cereal Special?
Whole Wheat
Whole wheat is an excellent everyday staple, supplying good-quality protein, dietary fibre, B-complex vitamins and several essential minerals. Because the bran and germ are retained, it also provides valuable antioxidant compounds that are largely lost during refining.
Khapli Wheat
Khapli wheat generally has one of the lowest glycemic indices among commonly consumed cereals. It also contains slightly more fibre, protein and several minerals than modern wheat, together with higher levels of naturally occurring antioxidants.
Jowar
Jowar is naturally gluten-free and stands out for its exceptionally rich antioxidant profile. These plant compounds may help reduce oxidative stress and chronic inflammation while contributing useful amounts of fibre and important minerals.
Bajri
Bajri combines dietary fibre with good amounts of iron, magnesium and protein, making it a nutrient-dense whole grain that provides sustained energy and supports overall nutritional balance.
Nachani (Ragi)
Ragi is unmatched among commonly eaten cereals for its calcium content and also provides fibre, magnesium and antioxidant compounds. However, despite its healthy reputation, finely milled ragi flour is not necessarily a low-glycemic food.
Processing Matters More Than Most People Realise
The way a grain is processed often has a greater impact on its effect on blood sugar than the grain itself.
Whole grains usually produce the lowest glycemic response.
Coarsely ground flour is generally preferable to finely milled flour.
Excessive grinding makes starch easier to digest, increasing the glycemic index.
Combining grains with pulses, vegetables, protein and healthy fats lowers the overall glycemic response of a meal.
Allowing cooked grains to cool before reheating increases resistant starch and may modestly reduce the glycemic response.
Which Cereal Comes Out on Top?
Lowest average glycemic index: Khapli wheat
Richest in antioxidants: Jowar
Highest calcium: Nachani (Ragi)
Highest iron: Bajri
Best all-round everyday staple: Whole wheat
Take-Home Message
Rather than searching for a single ‘super grain,’ it is wiser to appreciate the unique nutritional strengths of each. Whole wheat, khapli wheat, jowar, bajri and ragi all have an important place in a healthy diet.
Rotating different whole cereal through the week and combining them with pulses, soy foods, milk, curd, paneer, eggs, fish or lean meat, along with plenty of vegetables and healthy fats, provides a broader range of nutrients, improves overall diet quality and supports long-term metabolic health.
Related articles
Grid
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar!
Insulin – The Body’s Nutrient Gateway!
Most people think insulin exists only to lower blood sugar.
In reality, insulin has a much broader and far more important job.
Its main role is to help nutrients move from the bloodstream into body cells where they can be used or stored.
You can think of insulin as the body’s gateway hormone.
Without insulin, many cells cannot efficiently receive the nutrients they need.
Gateway For Glucose
After eating carbohydrates, digestion releases glucose into the bloodstream.
Blood glucose rises.
The pancreas responds by releasing insulin.
Insulin acts like a key that unlocks the doors of muscle cells and fat cells.
Glucose then enters these cells where it can be:
• used immediately to produce energy,
• stored as glycogen in muscles and the liver,
• or, when energy intake greatly exceeds requirements, eventually converted into body fat.
Without sufficient insulin—or when the body’s cells become resistant to insulin—glucose remains in the bloodstream and blood sugar rises.
Gateway For Amino Acids
The story is different after eating proteins.
Proteins are broken down into amino acids.
These amino acids also stimulate insulin release.
But this time insulin is not trying to lower blood sugar.
Instead, insulin helps amino acids enter muscle cells and other body tissues.
Once inside the cells, these amino acids are used to:
• build new muscle protein,
• repair damaged tissues,
• produce enzymes,
• manufacture hormones,
• support immune function.
Here, insulin functions as a growth and repair hormone rather than a glucose-lowering hormone.
Milk Demonstrates Both Roles Beautifully
Milk naturally contains both lactose and high-quality proteins.
The lactose produces a modest rise in blood glucose.
The proteins stimulate insulin through their amino acids.
Consequently, milk illustrates both major functions of insulin simultaneously.
Insulin helps glucose enter cells.
At the same time, it helps amino acids enter muscles for repair and maintenance.
Very few foods demonstrate both roles so clearly.
Exercise Makes The Gateway Work Better
Exercise opens another fascinating chapter.
When muscles contract during walking or strength training, they become much more responsive to insulin.
In other words, the gateway becomes easier to open.
The same amount of insulin can move more glucose and amino acids into muscle cells.
As a result:
• blood sugar rises less after meals,
• less insulin is needed,
• muscles receive more nutrients,
• muscle maintenance improves,
• metabolic health becomes better.
This is why regular physical activity improves insulin sensitivity.
When The Gateway Becomes Rusty
In insulin resistance, the gateway no longer responds efficiently.
The pancreas has to produce more and more insulin to achieve the same effect.
Over time, blood glucose begins to rise.
This is one of the earliest steps in the development of type 2 diabetes.
Fortunately, weight loss, regular walking, strength training and a healthy diet can often restore much of the gateway’s efficiency.
The Take-Home Message
Insulin is much more than a blood sugar hormone.
It is the body’s nutrient gateway.
It allows glucose to enter cells for energy.
It allows amino acids to enter cells for growth and repair.
Healthy muscles respond well to insulin.
Regular exercise keeps this gateway working efficiently.
Understanding insulin in this way makes it much easier to understand diabetes, muscle health, healthy ageing and nutrition.
Related article:
Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron and nachani (ragi) as the ideal calcium-rich grain.
The truth is that no single grain is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends on your overall diet, health goals and the way the grain is processed and prepared.
Comparison of Common Indian Cereals
***
Which Is the Healthiest Indian Cereal: Wheat, Khapli Wheat, Jowar, Bajri or Nachani?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli (Emmer) wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron, and nachani (ragi) as the ideal calcium-rich cereal.
The reality is more balanced. No single cereal is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends not only on the grain itself but also on your overall diet, health goals and how the grain is processed and prepared.
Comparison of Common Indian Cereals:
Whole Wheat
Glycemic Index: 50–60
Key Nutritional Strengths: Protein, fibre, B vitamins, magnesium, zinc and selenium.
Major Antioxidants: Ferulic acid, phenolic acids and lignans.
Khapli Wheat
Glycemic Index: 40–50
Key Nutritional Strengths: More fibre, slightly more protein, iron, magnesium and zinc than modern wheat.
Major Antioxidants: Polyphenols, lutein, carotenoids and ferulic acid.
Jowar
Glycemic Index: 55–65
Key Nutritional Strengths: Protein, fibre, magnesium, phosphorus and potassium.
Major Antioxidants: Anthocyanins, flavonoids, phenolic acids and tannins.
Bajri
Glycemic Index: 50–55
Key Nutritional Strengths: Protein, fibre, iron, magnesium and phosphorus.
Major Antioxidants: Phenolic acids, flavonoids and phytosterols.
Nachani (Ragi)
Glycemic Index: 60–70†
Key Nutritional Strengths: Exceptionally rich in calcium, fibre, magnesium and potassium.
Major Antioxidants: Polyphenols, ferulic acid, catechins and tannins.
Approximate glycemic index values that vary with processing and cooking.
Finely ground nachani (ragi) flour may have a higher glycemic index than commonly believed.
What Makes Each cereal Special?
Whole Wheat
Whole wheat is an excellent everyday staple, supplying good-quality protein, dietary fibre, B-complex vitamins and several essential minerals. Because the bran and germ are retained, it also provides valuable antioxidant compounds that are largely lost during refining.
Khapli Wheat
Khapli wheat generally has one of the lowest glycemic indices among commonly consumed cereals. It also contains slightly more fibre, protein and several minerals than modern wheat, together with higher levels of naturally occurring antioxidants.
Jowar
Jowar is naturally gluten-free and stands out for its exceptionally rich antioxidant profile. These plant compounds may help reduce oxidative stress and chronic inflammation while contributing useful amounts of fibre and important minerals.
Bajri
Bajri combines dietary fibre with good amounts of iron, magnesium and protein, making it a nutrient-dense whole grain that provides sustained energy and supports overall nutritional balance.
Nachani (Ragi)
Ragi is unmatched among commonly eaten cereals for its calcium content and also provides fibre, magnesium and antioxidant compounds. However, despite its healthy reputation, finely milled ragi flour is not necessarily a low-glycemic food.
Processing Matters More Than Most People Realise
The way a grain is processed often has a greater impact on its effect on blood sugar than the grain itself.
Whole grains usually produce the lowest glycemic response.
Coarsely ground flour is generally preferable to finely milled flour.
Excessive grinding makes starch easier to digest, increasing the glycemic index.
Combining grains with pulses, vegetables, protein and healthy fats lowers the overall glycemic response of a meal.
Allowing cooked grains to cool before reheating increases resistant starch and may modestly reduce the glycemic response.
Which Cereal Comes Out on Top?
Lowest average glycemic index: Khapli wheat
Richest in antioxidants: Jowar
Highest calcium: Nachani (Ragi)
Highest iron: Bajri
Best all-round everyday staple: Whole wheat
Take-Home Message
Rather than searching for a single ‘super grain,’ it is wiser to appreciate the unique nutritional strengths of each. Whole wheat, khapli wheat, jowar, bajri and ragi all have an important place in a healthy diet.
Rotating different whole cereal through the week and combining them with pulses, soy foods, milk, curd, paneer, eggs, fish or lean meat, along with plenty of vegetables and healthy fats, provides a broader range of nutrients, improves overall diet quality and supports long-term metabolic health.
Related articles

Milk And Paneer Vs Soya, Soya Milk And Tofu Proteins!
Milk Protein Vs Soya Protein: Which Is The Better Protein?
Protein is one of the most important nutrients for maintaining good health. It helps build muscles, repairs tissues, supports immunity, and keeps us feeling full after meals. However, not all protein sources are nutritionally identical. The amount of protein, the quality of that protein, and the calories that accompany it all influence how effectively a food supports muscle health.
Among the most commonly consumed protein foods for vegetarian people are milk, curds, buttermilk, and a combination of pulses and cereals, paneer is an occasional addition to their food.
And probably very few have soya, soya milk and tofu. Each has unique nutritional strengths and each has a place in a healthy diet.
Understanding Protein Quality
Proteins are made up of amino acids. Nine of these amino acids are called essential amino acids because the body cannot produce them and they must come from food.
A high-quality protein:
Contains all nine essential amino acids.
Is easily digested and absorbed.
Provides adequate amounts of the amino acid leucine, which plays a central role in stimulating muscle protein synthesis.
The higher the leucine content and the better the digestibility, the more efficiently the protein helps preserve and build muscle.
When muscle preservation is the primary goal, both protein quality and total daily protein intake matter.
Dairy Proteins
Milk is nature’s complete protein
Milk contains two proteins:
Casein (about 80%)
Whey (about 20%)
Both are complete, high-quality proteins.
Whey protein is rapidly absorbed and strongly stimulates muscle protein synthesis because it is naturally rich in leucine.
Casein is digested more slowly, providing a steady supply of amino acids over several hours and helping reduce muscle breakdown.
This combination makes milk one of the best natural foods for maintaining muscle mass.
Milk proteins (especially whey) produce the strongest immediate stimulation of muscle protein synthesis because they are rapidly digested and naturally rich in leucine.
For this reason, whey protein is often considered the gold standard for muscle building.
Soy Protein
Soy protein stimulates muscle protein synthesis almost as effectively.
Although its leucine content is slightly lower than whey, numerous clinical studies show that adequate soy protein intake successfully preserves muscle mass, particularly when combined with resistance exercise.
Current scientific evidence supports soy protein as the highest-quality plant protein available.
Comparing the Five Foods
All five foods provide excellent-quality protein and are highly effective for preserving muscle mass, but they differ in their protein concentration and calorie content.
Milk provides complete, high-quality protein with a moderate protein density and moderate calories, making it an ideal everyday protein source. Buffalo milk is even better in protein and calcium values than cow milk.
Whole cream paneer offers the same excellent-quality dairy protein in a much more concentrated form, although it contains more fat and hence more calories than milk. Its fat and calorie content can be reduced substantially by using low fat milk to prepare it.
Paneer is not a daily presence food in the Indian diet and is used as a occasional delicacy.
***
Whole grain soy flour is the most concentrated plant source of complete protein, apart from defatted soya flour, providing a high protein density (36 – 38 gm) but it is also high in fat (17.5- 21.5 gm) and calories (430 – 440 calories per 100 gm).
But we do not commonly eat it as we eat other pulses and legumes like toor (pigeon gram or red gram dal), whole mug and mug dal (green gram), chana dal or besan (Bengal dal or chickpeas), matki (moth bean), masur (lentil), chavali (black eyed peas or cow peas) or even the occasional chole (chickpeas) or rajma (red kidney beans) in curry or ‘usal’ form.
It is at most used as a small addition to wheat flour, by some families.
Tofu also provides excellent-quality complete protein but with a moderate protein density and the lowest calorie content among the five. It also is blood sugar and insulin neutral, meaning it causes minimal rise in blood sugar and insulin, making it particularly suitable for weight-loss diets, pre diabetics and diabetics and ladies with PCOS. But both, knowledge and public awareness of its availability and significance is low.
Natural soya milk lacks vitamin B12 and is low in calcium but fortified soya milk is on par with cow or toned milk in quality and quantity of protein and calcium and B12 content,
Only buffalo milk has higher protein and calcium content amongst dairy milk and soya milk.
When it comes to preserving muscle mass, all five foods are excellent choices, provided the overall daily protein intake is adequate and accompanied by regular strength-training exercise.
Which Should You Choose?
The best choice depends on your nutritional goals.
Milk
Excellent daily protein source
Ideal for children, adults and older people
Rich in calcium
Paneer
High-quality concentrated protein
Excellent in moderation
Higher in calories and saturated fat
The calorie and fat content is lower, while protein and calcium values are more less the same in low fat paneer.
Soybeans
Highest-quality plant protein
Rich in fibre and micronutrients
Particularly useful for vegetarians
High in fat and calorie content
Tofu
Lean, versatile and protein-rich
Lower in calories than paneer
It is blood sugar and insulin neutral
Excellent for weight loss, pre diabetes and diabetes and PCOS diets
The Bottom Line
Milk, curds, buttermilk and paneer, soybeans, soya milk and tofu are all valuable protein foods.
Milk and paneer provide outstanding dairy proteins, while soybeans, soy milk and tofu offer the best plant proteins available. Although whey protein stimulates muscle building slightly more strongly, well-planned diets containing adequate soy protein are highly effective at preserving muscle mass and supporting long-term health.
But it is difficult to see how soya and its products can replace milk and its products as they are culturally not our staple food.
For vegans, soya and its products could be a good alternative to milk and its products, if they can get used to their taste.
Rather than asking which is the ‘best,’ it is often wiser to include a variety of these protein-rich foods according to individual preferences, calorie requirements and health conditions.
Practical Take-Home Message
For vegetarians, there is no need to worry about inadequate protein quality if the diet regularly includes milk, curd or buttermilk, low fat paneer, and soy foods such as soybeans, soya milk or tofu.
While culturally milk and other dairy products are very much a part of our daily diet for generations, soya flour, or soya milk and tofu are not a part of our daily food. Plus it takes time to get used to the taste of soya products, especially soya milk and tofu.
Also soya milk is twice as expensive as the buffalo milk and even more so, than the cow milk. This is a serious drawback for average consumers.
Combined with regular strength-training exercise and adequate total protein intake, these foods can effectively help preserve muscle mass, support healthy ageing, and improve metabolic health.
Related articles
Medium
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar!
Insulin – The Body’s Nutrient Gateway!
Most people think insulin exists only to lower blood sugar.
In reality, insulin has a much broader and far more important job.
Its main role is to help nutrients move from the bloodstream into body cells where they can be used or stored.
You can think of insulin as the body’s gateway hormone.
Without insulin, many cells cannot efficiently receive the nutrients they need.
Gateway For Glucose
After eating carbohydrates, digestion releases glucose into the bloodstream.
Blood glucose rises.
The pancreas responds by releasing insulin.
Insulin acts like a key that unlocks the doors of muscle cells and fat cells.
Glucose then enters these cells where it can be:
• used immediately to produce energy,
• stored as glycogen in muscles and the liver,
• or, when energy intake greatly exceeds requirements, eventually converted into body fat.
Without sufficient insulin—or when the body’s cells become resistant to insulin—glucose remains in the bloodstream and blood sugar rises.
Gateway For Amino Acids
The story is different after eating proteins.
Proteins are broken down into amino acids.
These amino acids also stimulate insulin release.
But this time insulin is not trying to lower blood sugar.
Instead, insulin helps amino acids enter muscle cells and other body tissues.
Once inside the cells, these amino acids are used to:
• build new muscle protein,
• repair damaged tissues,
• produce enzymes,
• manufacture hormones,
• support immune function.
Here, insulin functions as a growth and repair hormone rather than a glucose-lowering hormone.
Milk Demonstrates Both Roles Beautifully
Milk naturally contains both lactose and high-quality proteins.
The lactose produces a modest rise in blood glucose.
The proteins stimulate insulin through their amino acids.
Consequently, milk illustrates both major functions of insulin simultaneously.
Insulin helps glucose enter cells.
At the same time, it helps amino acids enter muscles for repair and maintenance.
Very few foods demonstrate both roles so clearly.
Exercise Makes The Gateway Work Better
Exercise opens another fascinating chapter.
When muscles contract during walking or strength training, they become much more responsive to insulin.
In other words, the gateway becomes easier to open.
The same amount of insulin can move more glucose and amino acids into muscle cells.
As a result:
• blood sugar rises less after meals,
• less insulin is needed,
• muscles receive more nutrients,
• muscle maintenance improves,
• metabolic health becomes better.
This is why regular physical activity improves insulin sensitivity.
When The Gateway Becomes Rusty
In insulin resistance, the gateway no longer responds efficiently.
The pancreas has to produce more and more insulin to achieve the same effect.
Over time, blood glucose begins to rise.
This is one of the earliest steps in the development of type 2 diabetes.
Fortunately, weight loss, regular walking, strength training and a healthy diet can often restore much of the gateway’s efficiency.
The Take-Home Message
Insulin is much more than a blood sugar hormone.
It is the body’s nutrient gateway.
It allows glucose to enter cells for energy.
It allows amino acids to enter cells for growth and repair.
Healthy muscles respond well to insulin.
Regular exercise keeps this gateway working efficiently.
Understanding insulin in this way makes it much easier to understand diabetes, muscle health, healthy ageing and nutrition.
Related article:

Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron and nachani (ragi) as the ideal calcium-rich grain.
The truth is that no single grain is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends on your overall diet, health goals and the way the grain is processed and prepared.
Comparison of Common Indian Cereals
***
Which Is the Healthiest Indian Cereal: Wheat, Khapli Wheat, Jowar, Bajri or Nachani?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli (Emmer) wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron, and nachani (ragi) as the ideal calcium-rich cereal.
The reality is more balanced. No single cereal is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends not only on the grain itself but also on your overall diet, health goals and how the grain is processed and prepared.
Comparison of Common Indian Cereals:
Whole Wheat
Glycemic Index: 50–60
Key Nutritional Strengths: Protein, fibre, B vitamins, magnesium, zinc and selenium.
Major Antioxidants: Ferulic acid, phenolic acids and lignans.
Khapli Wheat
Glycemic Index: 40–50
Key Nutritional Strengths: More fibre, slightly more protein, iron, magnesium and zinc than modern wheat.
Major Antioxidants: Polyphenols, lutein, carotenoids and ferulic acid.
Jowar
Glycemic Index: 55–65
Key Nutritional Strengths: Protein, fibre, magnesium, phosphorus and potassium.
Major Antioxidants: Anthocyanins, flavonoids, phenolic acids and tannins.
Bajri
Glycemic Index: 50–55
Key Nutritional Strengths: Protein, fibre, iron, magnesium and phosphorus.
Major Antioxidants: Phenolic acids, flavonoids and phytosterols.
Nachani (Ragi)
Glycemic Index: 60–70†
Key Nutritional Strengths: Exceptionally rich in calcium, fibre, magnesium and potassium.
Major Antioxidants: Polyphenols, ferulic acid, catechins and tannins.
Approximate glycemic index values that vary with processing and cooking.
Finely ground nachani (ragi) flour may have a higher glycemic index than commonly believed.
What Makes Each cereal Special?
Whole Wheat
Whole wheat is an excellent everyday staple, supplying good-quality protein, dietary fibre, B-complex vitamins and several essential minerals. Because the bran and germ are retained, it also provides valuable antioxidant compounds that are largely lost during refining.
Khapli Wheat
Khapli wheat generally has one of the lowest glycemic indices among commonly consumed cereals. It also contains slightly more fibre, protein and several minerals than modern wheat, together with higher levels of naturally occurring antioxidants.
Jowar
Jowar is naturally gluten-free and stands out for its exceptionally rich antioxidant profile. These plant compounds may help reduce oxidative stress and chronic inflammation while contributing useful amounts of fibre and important minerals.
Bajri
Bajri combines dietary fibre with good amounts of iron, magnesium and protein, making it a nutrient-dense whole grain that provides sustained energy and supports overall nutritional balance.
Nachani (Ragi)
Ragi is unmatched among commonly eaten cereals for its calcium content and also provides fibre, magnesium and antioxidant compounds. However, despite its healthy reputation, finely milled ragi flour is not necessarily a low-glycemic food.
Processing Matters More Than Most People Realise
The way a grain is processed often has a greater impact on its effect on blood sugar than the grain itself.
Whole grains usually produce the lowest glycemic response.
Coarsely ground flour is generally preferable to finely milled flour.
Excessive grinding makes starch easier to digest, increasing the glycemic index.
Combining grains with pulses, vegetables, protein and healthy fats lowers the overall glycemic response of a meal.
Allowing cooked grains to cool before reheating increases resistant starch and may modestly reduce the glycemic response.
Which Cereal Comes Out on Top?
Lowest average glycemic index: Khapli wheat
Richest in antioxidants: Jowar
Highest calcium: Nachani (Ragi)
Highest iron: Bajri
Best all-round everyday staple: Whole wheat
Take-Home Message
Rather than searching for a single ‘super grain,’ it is wiser to appreciate the unique nutritional strengths of each. Whole wheat, khapli wheat, jowar, bajri and ragi all have an important place in a healthy diet.
Rotating different whole cereal through the week and combining them with pulses, soy foods, milk, curd, paneer, eggs, fish or lean meat, along with plenty of vegetables and healthy fats, provides a broader range of nutrients, improves overall diet quality and supports long-term metabolic health.
Related articles
Large
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar!
Insulin – The Body’s Nutrient Gateway!
Most people think insulin exists only to lower blood sugar.
In reality, insulin has a much broader and far more important job.
Its main role is to help nutrients move from the bloodstream into body cells where they can be used or stored.
You can think of insulin as the body’s gateway hormone.
Without insulin, many cells cannot efficiently receive the nutrients they need.
Gateway For Glucose
After eating carbohydrates, digestion releases glucose into the bloodstream.
Blood glucose rises.
The pancreas responds by releasing insulin.
Insulin acts like a key that unlocks the doors of muscle cells and fat cells.
Glucose then enters these cells where it can be:
• used immediately to produce energy,
• stored as glycogen in muscles and the liver,
• or, when energy intake greatly exceeds requirements, eventually converted into body fat.
Without sufficient insulin—or when the body’s cells become resistant to insulin—glucose remains in the bloodstream and blood sugar rises.
Gateway For Amino Acids
The story is different after eating proteins.
Proteins are broken down into amino acids.
These amino acids also stimulate insulin release.
But this time insulin is not trying to lower blood sugar.
Instead, insulin helps amino acids enter muscle cells and other body tissues.
Once inside the cells, these amino acids are used to:
• build new muscle protein,
• repair damaged tissues,
• produce enzymes,
• manufacture hormones,
• support immune function.
Here, insulin functions as a growth and repair hormone rather than a glucose-lowering hormone.
Milk Demonstrates Both Roles Beautifully
Milk naturally contains both lactose and high-quality proteins.
The lactose produces a modest rise in blood glucose.
The proteins stimulate insulin through their amino acids.
Consequently, milk illustrates both major functions of insulin simultaneously.
Insulin helps glucose enter cells.
At the same time, it helps amino acids enter muscles for repair and maintenance.
Very few foods demonstrate both roles so clearly.
Exercise Makes The Gateway Work Better
Exercise opens another fascinating chapter.
When muscles contract during walking or strength training, they become much more responsive to insulin.
In other words, the gateway becomes easier to open.
The same amount of insulin can move more glucose and amino acids into muscle cells.
As a result:
• blood sugar rises less after meals,
• less insulin is needed,
• muscles receive more nutrients,
• muscle maintenance improves,
• metabolic health becomes better.
This is why regular physical activity improves insulin sensitivity.
When The Gateway Becomes Rusty
In insulin resistance, the gateway no longer responds efficiently.
The pancreas has to produce more and more insulin to achieve the same effect.
Over time, blood glucose begins to rise.
This is one of the earliest steps in the development of type 2 diabetes.
Fortunately, weight loss, regular walking, strength training and a healthy diet can often restore much of the gateway’s efficiency.
The Take-Home Message
Insulin is much more than a blood sugar hormone.
It is the body’s nutrient gateway.
It allows glucose to enter cells for energy.
It allows amino acids to enter cells for growth and repair.
Healthy muscles respond well to insulin.
Regular exercise keeps this gateway working efficiently.
Understanding insulin in this way makes it much easier to understand diabetes, muscle health, healthy ageing and nutrition.
Related article:
Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron and nachani (ragi) as the ideal calcium-rich grain.
The truth is that no single grain is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends on your overall diet, health goals and the way the grain is processed and prepared.
Comparison of Common Indian Cereals
***
Which Is the Healthiest Indian Cereal: Wheat, Khapli Wheat, Jowar, Bajri or Nachani?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli (Emmer) wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron, and nachani (ragi) as the ideal calcium-rich cereal.
The reality is more balanced. No single cereal is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends not only on the grain itself but also on your overall diet, health goals and how the grain is processed and prepared.
Comparison of Common Indian Cereals:
Whole Wheat
Glycemic Index: 50–60
Key Nutritional Strengths: Protein, fibre, B vitamins, magnesium, zinc and selenium.
Major Antioxidants: Ferulic acid, phenolic acids and lignans.
Khapli Wheat
Glycemic Index: 40–50
Key Nutritional Strengths: More fibre, slightly more protein, iron, magnesium and zinc than modern wheat.
Major Antioxidants: Polyphenols, lutein, carotenoids and ferulic acid.
Jowar
Glycemic Index: 55–65
Key Nutritional Strengths: Protein, fibre, magnesium, phosphorus and potassium.
Major Antioxidants: Anthocyanins, flavonoids, phenolic acids and tannins.
Bajri
Glycemic Index: 50–55
Key Nutritional Strengths: Protein, fibre, iron, magnesium and phosphorus.
Major Antioxidants: Phenolic acids, flavonoids and phytosterols.
Nachani (Ragi)
Glycemic Index: 60–70†
Key Nutritional Strengths: Exceptionally rich in calcium, fibre, magnesium and potassium.
Major Antioxidants: Polyphenols, ferulic acid, catechins and tannins.
Approximate glycemic index values that vary with processing and cooking.
Finely ground nachani (ragi) flour may have a higher glycemic index than commonly believed.
What Makes Each cereal Special?
Whole Wheat
Whole wheat is an excellent everyday staple, supplying good-quality protein, dietary fibre, B-complex vitamins and several essential minerals. Because the bran and germ are retained, it also provides valuable antioxidant compounds that are largely lost during refining.
Khapli Wheat
Khapli wheat generally has one of the lowest glycemic indices among commonly consumed cereals. It also contains slightly more fibre, protein and several minerals than modern wheat, together with higher levels of naturally occurring antioxidants.
Jowar
Jowar is naturally gluten-free and stands out for its exceptionally rich antioxidant profile. These plant compounds may help reduce oxidative stress and chronic inflammation while contributing useful amounts of fibre and important minerals.
Bajri
Bajri combines dietary fibre with good amounts of iron, magnesium and protein, making it a nutrient-dense whole grain that provides sustained energy and supports overall nutritional balance.
Nachani (Ragi)
Ragi is unmatched among commonly eaten cereals for its calcium content and also provides fibre, magnesium and antioxidant compounds. However, despite its healthy reputation, finely milled ragi flour is not necessarily a low-glycemic food.
Processing Matters More Than Most People Realise
The way a grain is processed often has a greater impact on its effect on blood sugar than the grain itself.
Whole grains usually produce the lowest glycemic response.
Coarsely ground flour is generally preferable to finely milled flour.
Excessive grinding makes starch easier to digest, increasing the glycemic index.
Combining grains with pulses, vegetables, protein and healthy fats lowers the overall glycemic response of a meal.
Allowing cooked grains to cool before reheating increases resistant starch and may modestly reduce the glycemic response.
Which Cereal Comes Out on Top?
Lowest average glycemic index: Khapli wheat
Richest in antioxidants: Jowar
Highest calcium: Nachani (Ragi)
Highest iron: Bajri
Best all-round everyday staple: Whole wheat
Take-Home Message
Rather than searching for a single ‘super grain,’ it is wiser to appreciate the unique nutritional strengths of each. Whole wheat, khapli wheat, jowar, bajri and ragi all have an important place in a healthy diet.
Rotating different whole cereal through the week and combining them with pulses, soy foods, milk, curd, paneer, eggs, fish or lean meat, along with plenty of vegetables and healthy fats, provides a broader range of nutrients, improves overall diet quality and supports long-term metabolic health.
Related articles
Large Alt
Insulin – The Body’s Nutrient Gateway!
Insulin Doesn’t Just Regulate Blood Sugar!
Insulin – The Body’s Nutrient Gateway!
Most people think insulin exists only to lower blood sugar.
In reality, insulin has a much broader and far more important job.
Its main role is to help nutrients move from the bloodstream into body cells where they can be used or stored.
You can think of insulin as the body’s gateway hormone.
Without insulin, many cells cannot efficiently receive the nutrients they need.
Gateway For Glucose
After eating carbohydrates, digestion releases glucose into the bloodstream.
Blood glucose rises.
The pancreas responds by releasing insulin.
Insulin acts like a key that unlocks the doors of muscle cells and fat cells.
Glucose then enters these cells where it can be:
• used immediately to produce energy,
• stored as glycogen in muscles and the liver,
• or, when energy intake greatly exceeds requirements, eventually converted into body fat.
Without sufficient insulin—or when the body’s cells become resistant to insulin—glucose remains in the bloodstream and blood sugar rises.
Gateway For Amino Acids
The story is different after eating proteins.
Proteins are broken down into amino acids.
These amino acids also stimulate insulin release.
But this time insulin is not trying to lower blood sugar.
Instead, insulin helps amino acids enter muscle cells and other body tissues.
Once inside the cells, these amino acids are used to:
• build new muscle protein,
• repair damaged tissues,
• produce enzymes,
• manufacture hormones,
• support immune function.
Here, insulin functions as a growth and repair hormone rather than a glucose-lowering hormone.
Milk Demonstrates Both Roles Beautifully
Milk naturally contains both lactose and high-quality proteins.
The lactose produces a modest rise in blood glucose.
The proteins stimulate insulin through their amino acids.
Consequently, milk illustrates both major functions of insulin simultaneously.
Insulin helps glucose enter cells.
At the same time, it helps amino acids enter muscles for repair and maintenance.
Very few foods demonstrate both roles so clearly.
Exercise Makes The Gateway Work Better
Exercise opens another fascinating chapter.
When muscles contract during walking or strength training, they become much more responsive to insulin.
In other words, the gateway becomes easier to open.
The same amount of insulin can move more glucose and amino acids into muscle cells.
As a result:
• blood sugar rises less after meals,
• less insulin is needed,
• muscles receive more nutrients,
• muscle maintenance improves,
• metabolic health becomes better.
This is why regular physical activity improves insulin sensitivity.
When The Gateway Becomes Rusty
In insulin resistance, the gateway no longer responds efficiently.
The pancreas has to produce more and more insulin to achieve the same effect.
Over time, blood glucose begins to rise.
This is one of the earliest steps in the development of type 2 diabetes.
Fortunately, weight loss, regular walking, strength training and a healthy diet can often restore much of the gateway’s efficiency.
The Take-Home Message
Insulin is much more than a blood sugar hormone.
It is the body’s nutrient gateway.
It allows glucose to enter cells for energy.
It allows amino acids to enter cells for growth and repair.
Healthy muscles respond well to insulin.
Regular exercise keeps this gateway working efficiently.
Understanding insulin in this way makes it much easier to understand diabetes, muscle health, healthy ageing and nutrition.
Related article:
Which Is The Healthiest Indian Cereal?
Wheat, Khapli Wheat, Jowar, Bajri or Nachani: Which Is The Healthiest Cereal?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron and nachani (ragi) as the ideal calcium-rich grain.
The truth is that no single grain is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends on your overall diet, health goals and the way the grain is processed and prepared.
Comparison of Common Indian Cereals
***
Which Is the Healthiest Indian Cereal: Wheat, Khapli Wheat, Jowar, Bajri or Nachani?
Walk through any supermarket or browse social media, and you’ll find claims that one grain is healthier than all the others. Khapli (Emmer) wheat is promoted as diabetic-friendly, jowar as an antioxidant powerhouse, bajri as rich in iron, and nachani (ragi) as the ideal calcium-rich cereal.
The reality is more balanced. No single cereal is nutritionally superior in every respect. Each has its own strengths, and the healthiest choice depends not only on the grain itself but also on your overall diet, health goals and how the grain is processed and prepared.
Comparison of Common Indian Cereals:
Whole Wheat
Glycemic Index: 50–60
Key Nutritional Strengths: Protein, fibre, B vitamins, magnesium, zinc and selenium.
Major Antioxidants: Ferulic acid, phenolic acids and lignans.
Khapli Wheat
Glycemic Index: 40–50
Key Nutritional Strengths: More fibre, slightly more protein, iron, magnesium and zinc than modern wheat.
Major Antioxidants: Polyphenols, lutein, carotenoids and ferulic acid.
Jowar
Glycemic Index: 55–65
Key Nutritional Strengths: Protein, fibre, magnesium, phosphorus and potassium.
Major Antioxidants: Anthocyanins, flavonoids, phenolic acids and tannins.
Bajri
Glycemic Index: 50–55
Key Nutritional Strengths: Protein, fibre, iron, magnesium and phosphorus.
Major Antioxidants: Phenolic acids, flavonoids and phytosterols.
Nachani (Ragi)
Glycemic Index: 60–70†
Key Nutritional Strengths: Exceptionally rich in calcium, fibre, magnesium and potassium.
Major Antioxidants: Polyphenols, ferulic acid, catechins and tannins.
Approximate glycemic index values that vary with processing and cooking.
Finely ground nachani (ragi) flour may have a higher glycemic index than commonly believed.
What Makes Each cereal Special?
Whole Wheat
Whole wheat is an excellent everyday staple, supplying good-quality protein, dietary fibre, B-complex vitamins and several essential minerals. Because the bran and germ are retained, it also provides valuable antioxidant compounds that are largely lost during refining.
Khapli Wheat
Khapli wheat generally has one of the lowest glycemic indices among commonly consumed cereals. It also contains slightly more fibre, protein and several minerals than modern wheat, together with higher levels of naturally occurring antioxidants.
Jowar
Jowar is naturally gluten-free and stands out for its exceptionally rich antioxidant profile. These plant compounds may help reduce oxidative stress and chronic inflammation while contributing useful amounts of fibre and important minerals.
Bajri
Bajri combines dietary fibre with good amounts of iron, magnesium and protein, making it a nutrient-dense whole grain that provides sustained energy and supports overall nutritional balance.
Nachani (Ragi)
Ragi is unmatched among commonly eaten cereals for its calcium content and also provides fibre, magnesium and antioxidant compounds. However, despite its healthy reputation, finely milled ragi flour is not necessarily a low-glycemic food.
Processing Matters More Than Most People Realise
The way a grain is processed often has a greater impact on its effect on blood sugar than the grain itself.
Whole grains usually produce the lowest glycemic response.
Coarsely ground flour is generally preferable to finely milled flour.
Excessive grinding makes starch easier to digest, increasing the glycemic index.
Combining grains with pulses, vegetables, protein and healthy fats lowers the overall glycemic response of a meal.
Allowing cooked grains to cool before reheating increases resistant starch and may modestly reduce the glycemic response.
Which Cereal Comes Out on Top?
Lowest average glycemic index: Khapli wheat
Richest in antioxidants: Jowar
Highest calcium: Nachani (Ragi)
Highest iron: Bajri
Best all-round everyday staple: Whole wheat
Take-Home Message
Rather than searching for a single ‘super grain,’ it is wiser to appreciate the unique nutritional strengths of each. Whole wheat, khapli wheat, jowar, bajri and ragi all have an important place in a healthy diet.
Rotating different whole cereal through the week and combining them with pulses, soy foods, milk, curd, paneer, eggs, fish or lean meat, along with plenty of vegetables and healthy fats, provides a broader range of nutrients, improves overall diet quality and supports long-term metabolic health.
Related articles